41 YEAR OLD MALE WITH ITCHING AND SCALING LESIONS
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your
valuable comments on comment box is welcome
CASE:
41 year old male came with the chief complaints of itching and scaling of skin all over the body since the last two months
HISTORY OF PRESENTING ILLNESS
The patient was apparently asymptomatic 25 years ago then he developed itching and scaling over the scalp which then spread to his face, shoulders, chest, abdomen, back and lower limbs involving the whole body. He went to a dermatologists then and was given medication but it did not reduce, so over the years he has tried different medications including homeopathy and ayurveda and then the itching and scaling reduced with recurrent episodes over the years.
7 years ago while he was working as a courier delivery man he was exposed to heavy rain which increased his condition he immediately went to a local RMP who gave him an injection of dexamethosone and triamsinalone which relieved his symptoms immediately within one hour. Since then he has been visiting the same clinic and has been taking these injections every two to three since then. 3 months ago he developed an infection at the injection site (right thigh).
It progressed with a yellow discharge (pus) coming from the site which then reduced spontaneously without any medication. Then he continued the injections given by the rmp but this time the itching and scaling did not reduce. He has also lost 15 kgs in this period.
He also has weakness (unable to stand for longer periods, pain in legs after walking) since 3 months and pedal edema since three months which was of pitting type. Since his health has deteriorated in the last 3 months he went to a doctor 7 days ago and then was referred to our hospital for further testing.

PAST HISTORY:
He is not a known case of diabetes, hypertension, asthama, tuberculosis
Has no history of any previous surgeries
FAMILY HISTORY
His maternal uncle has a history of similar complainfs
PERSONAL HISTORY:
Diet: vegetarian since the last 10 years
Appetite: decreased since the last 3 months
Sleep: inadequate as he stays awake at night due to the itching
Bowel and bladder : regular
Addictions: drinks 90ml of alcohol since 15 years, drinks everyday for a few weeks and then discontinues for a while.
Consumes 1 packet of tobacco everyday.
DAILY ROUTINE:
The patient had to change many occupations over the years due to his health. Initially he was a courier delivery man but had to leave the job as his condition worsened depending on the weather. He is currently a painter.
He daily wakes up at 7 am in the morning and does his morning hygiene routie following which he goes to work if he has or else he stays at home. He comes in the evening and drinks regularly. He is unable to fall asleep as he feels discomfort and usually peels the scaly skin due to itching. He falls asleep early in the morning.
MEDICATION HISTORY:
Methotrexate, propysalic ointment, betamethasone, homeopathy and ayurveda since the last 10 years (irregular)
Inj. Dexamethasone/kenocort every 3 months since the last 7 years.
GENERAL EXAMIANTION:
On examination
Patient conscious, coherent, cooperative
Pallor present
No icterus, cyanosis, clubbing, lymphadenopathy, Edema
Scaly lesions present all over the body
Vitals:
Temperature:101
BP: 100/70 mm of Hg
Pulse rate: 96
Respiratory rate: 24
GRBS: 96mg/dl







SYSTEMIC EXAMINATION:
1) CVS:
S1 and S2 heard
No thrills and murmurs
2) RESPIRATORY SYSTEM:
Inspection: no scars, equal bilateral chest expansion,
Percussion: resonant in all areas
Palpation: trachea centrally placed, bilateral expansion of chest is equal
Ausculation: vesicular breath sounds heard in all areas
3)ABDOMEN;
flat abdomen, no scars , scaling all over the skin, no hepatomegaly and spleenomegaly
No tenderness present
4)CNS:
Patient is conscious and alert
Speech is normal
Cranial nerves: 1-12 : normal
Sensory examination: normal
Motor examinatio: tone: normal
Power : 5/5 (normal)
Reflexes: all reflesxes: +3
PROVISIONAL DIAGNOSIS:
Erythrodermic psoriasis
INVESTIGATIONS:
HAEMOGLOBIN : 10.1gm/dl
RFT:
Creatinine: 0.4md/dl
ESR: 26 mm/1st hour
LFT:
Total bilirubin: 1.05 mg/dl
Alkaline phosphate: 318 IU/L
Total proteins: 6.1 gm/dl
Albumin: 2.5gm/dl






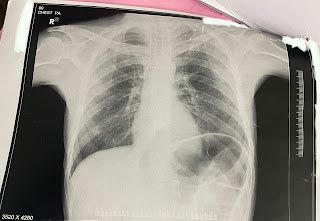
Chest Xray-
TREATMENT:
1) liquid paraffin+glycerin+water (apply in equal proportions) three times/day
2)tab atarax 25mg OD
3) tab shelcal OD
4)protein x powder with milk
5) high protein diet
6) tab MVT OD
7) tab pregabalin 75mg + tab methylcobalamine 750mcg


Comments
Post a Comment